You may have noticed the Supreme Court announced several crucial rulings on controversial topics. Buried in most coverage was a note that the Court upheld the legality of the U.S. Preventive Services Task Force (USPSTF).
Most folks have no clue what the USPSTF is or does. To people like me, it is crucial to advancing the early detection and prevention of cancer in the United States. For now, we can be grateful that the Task Force is “safe” from immediate elimination.
The bottom line is that the USPSTF is now affirmed as a lawful committee brought together under the auspices of Secretary Kennedy, as noted by the Court.
Before we celebrate too much, we should be aware that a victory today does not mean survival tomorrow. That which Secretary Kennedy brings together is also something Secretary Kennedy can tear apart. He has done that recently with the vaccine folks, so I doubt there is much to prevent him from doing the same for the Task Force.
I am concerned that the powers in charge may focus on other ways to gut the Task Force and drive a different wedge into the effectiveness of the Affordable Care Act (ACA). Viewed through that lens, preventive care as part of the ACA is vulnerable.
The Task Force’s key function is to evaluate which preventive medical services have sufficient evidence to be widely applied in preventive care, and which services do not have sufficient evidence to warrant coverage or should not be generally employed in the routine care of patients by primary care clinicians.
When the Task Force gives its blessing, insurers must provide those screenings at no charge to patients. If there is no blessing, then coverage is not required. That does not mean insurers won’t cover the service, just that they are not required to do so. Think of the Task Force recommendations as a floor, not a ceiling.
In the world of evidence-based cancer screening, cervical cancer, mammography, BRCA tests, and colorectal cancer screening make the cut. Prostate cancer screening does not.
Making these preventive health services available at no cost is a big deal. What gets covered and paid gets done; what is not covered is less likely to be done. Patients do not exactly have a lot of extra cash lying around to pay for medical services with large copays, deductibles, or no insurance coverage these days.
Finding cancer “early” usually means better outcomes, with less intense treatments. There is undoubtedly overdiagnosis of cancers through screening—meaning that we find cancers that do not have to be found (perhaps more on that topic another day). Notwithstanding overdiagnosis of cancer, the reality is we are doing better when it comes to reducing deaths from cancer.
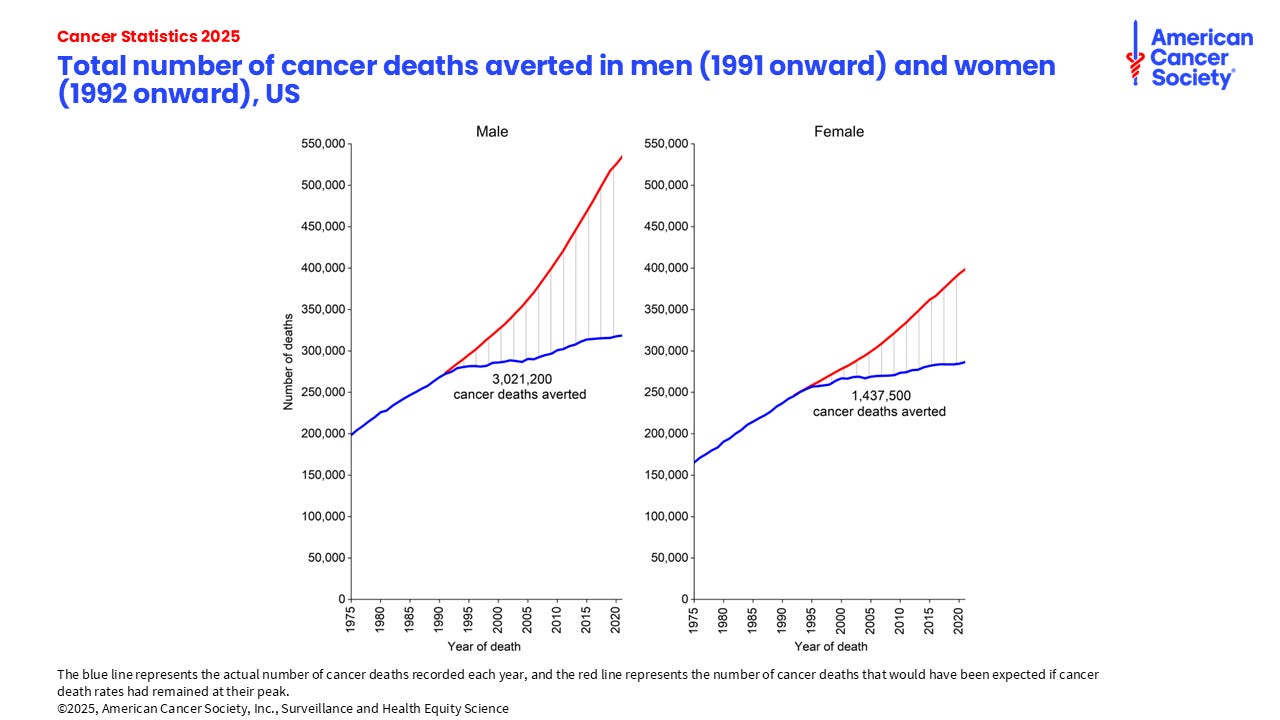
While screening is not the sole reason for that decline, it is an important contributor. Millions of folks have avoided premature deaths from cancer because of our progress, as shown in this data from the American Cancer Society:
Prior to the ACA mandating nationwide insurance coverage for cancer screening, it was each state for itself when it came to policies on whether—and which—cancer screenings would be covered by insurance.
Organizations like the American Cancer Society devoted substantial resources encouraging state legislators to cover tests like mammograms and colonoscopies. Some states said yes, others said no. It was a food fight between citizens, the insurers, and the employers. Notwithstanding the lives that could be saved, many employers and insurers did not want to pay the cost of cancer prevention, as modest as the cost was at the time.
Enter the passage of the ACA in March 2010 and the Task Force became the “deemed nationwide authority” to make the decisions on coverage for cancer prevention and other preventive health measures. There is little question in my mind that we have all benefitted from that opportunity.
As mentioned at the beginning, just because the Court ruled that the Task Force and the ACA were safe for now does not mean they will be safe forever. The final decision has yet to be made.
It is no secret that over the years, the Republicans have made several attempts to disband the ACA. At least this time, the administration agreed to come down on the side of the Task Force in the current case. Good for them. It was the right thing to do.
But time has a way of whittling away at good intentions, and the ACA is no different.
The Medicaid debate currently underway in Washington is a good example: There is a lot of “top line” public discussion about how much the current budget legislation will cut Medicaid coverage. There is much less attention paid to the more nuanced, unexpected consequences of those cuts that may be buried in the bill. We shall see this week what happens.
Meanwhile, back at the ranch, I am concerned the administration—especially given Secretary Kennedy’s recent actions disbanding and reconstituting the vaccine advisory panel with folks more to his liking—will someday in the not too distant future turn its focus to the Task Force in a similar fashion.
There are strong forces at work in Washington these days—patient forces (meaning they are patient and willing to take their time to meet their objectives, not patients who seek medical care)—who do not like the ACA for a variety of reasons. And the same ruling that gave the Task Force a reprieve could also be used against it.
The current ruling established that the Task Force is a committee that is under the control of the administration. That means the Secretary of Health and Human Services plays a crucial role in appointing and overseeing the actions of the Task Force. And what the Secretary giveth can certainly be taken away, just as he did with the vaccine folks.
There is another wrinkle, one that I am surprised did not happen during the heyday of the DOGE efforts:
While the Task Force is an independent committee, the Secretary could decide to disband the agency that supports the Task Force as part of his effort to reduce the budget of HHS. That agency is called the Agency for Health Care Research and Quality, or AHRQ for short.
AHRQ does a lot of good work, but so did the Agency for International Development (AID). We know what happened to them, do not we? There is nothing protecting the good work of AHRQ either. They could be vulnerable as Kennedy and Co. get their feet on the ground and focus on other “opportunities” to downsize HHS down the road.
I would be more comfortable if Kennedy, MAHA, and others had a clue about how to genuinely improve the public’s health. But from my vantage point, as previously discussed, they are out to lunch when it comes to actually improving the health of America.
The things that MAHA worries about most will not move the needle on the health of Americans. And that means they may not embrace spending necessary funds on agencies like AHRQ or committees like the USPSTF.
The Task Force is already under resourced and having difficulty doing the work it needs to do on prevention guidelines. It takes a long time for them to gather the evidence and make and/or update their recommendations. Industry is complaining loudly about the impact of those delays on moving new prevention technologies forward into the public arena, such as blood-based screening for colon and other cancers. (In disclosure, I have been a paid advisor for one of those companies, Guardant Health, and also sat on a committee that was convened to provide information to the public about the role of these technologies. That committee was funded in part by industry.)
With funding in short supply, my fear is that it would not be a giant step for the Secretary to either eliminate the overarching agency (AHRQ) or gut the Task Force itself and replace it with folks who want to promote consumption of unpasteurized milk or extol the impact of removing food dyes from our food supply as primary approaches to improving public health and preventing disease.
I do not know what such a move would mean for the Affordable Care Act writ large, but I do know it would gut the prevention programs, since alternatives to the Task Force as an arbiter of coverage simply do not exist, and reconstituting such an oversight committee would not be a simple task. Not to mention that it would literally take an act of Congress to provide such authority regarding cancer prevention to a different entity other than the Task Force—and such actions are a bit unlikely these days.
As a new week begins, some will take comfort that all remains intact on the prevention front. I hope it stays that way.
You want to preserve the public’s health? Then hands off the Task Force, and hands off proven and effective prevention strategies. My fear is that in these unsettled times Mr. Kennedy will find more ways to damage our health rather than improve it.
“Thoughts and prayers” and Supreme Court decisions are helpful.
The question remains: Will they be enough?
J. Leonard Lichtenfeld is an oncologist.



































