Working the night shift is brutal. Circadian rhythms are disrupted, backup help in true emergencies is limited, and even simple things like labs or imaging can take far longer than they should. But one of the biggest challenges is late-night snacking.
There is something about the combination of darkness, fatigue, and intermittent slow periods that makes it ridiculously easy to inhale a two-pound bag of potato chips without thinking twice. Research shows that sleep deprivation alters ghrelin and leptin levels, raising hunger signals while blunting satiety. Add a long overnight shift, and it is no surprise that weight gain is common among night-shift physicians.
I had heard a lot about intermittent fasting, with some people narrowing their “eating window” to as little as six hours. I wanted something more practical. So I created a simple rule: No eating from 8:00 p.m. until 1:00 a.m. Other than that one rule, I made no changes to my diet or lifestyle. Water, coffee, and diet soda were allowed during the fasting window.
I anticipated that early changes would be subtle, so I began with weekly weigh-ins. After two weeks, I transitioned to near-daily weigh-ins, always at the same time, on the same scale, in the same spot on my bathroom floor. Data were collected over eight weeks.
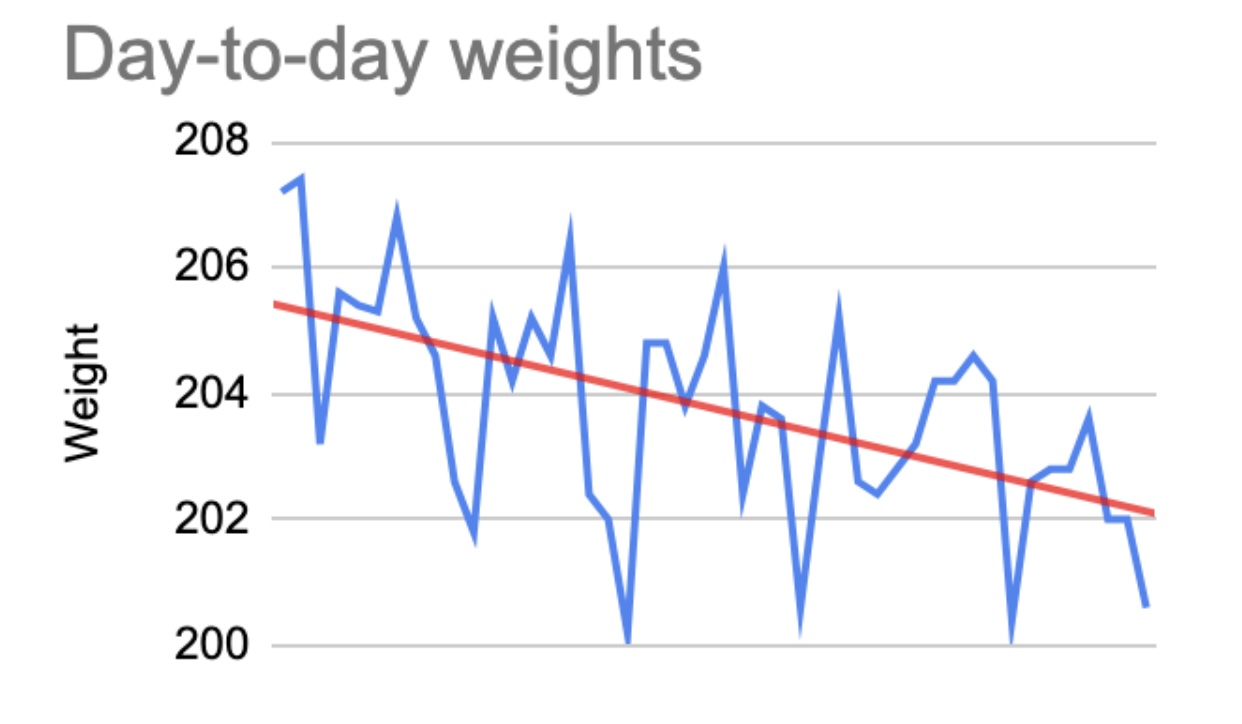
Results and day-to-day volatility
Approximately 40 weigh-ins were recorded during the study period. Daily weights fluctuated significantly, sometimes by several pounds from one day to the next. Frustrating? Absolutely. Expected? Also yes. These swings likely reflect normal physiologic variation, such as fluid shifts, glycogen storage, sodium intake, and gastrointestinal contents, rather than true changes in body fat.
Smoothed weight trends
To better understand the underlying trajectory, seven-day rolling averages were calculated:
- Late December: ~207.2 lbs
- Early January: ~205 to 206 lbs
- Mid-January: ~203.5 to 204.5 lbs
- Early February: ~203.0 lbs
- Late February: ~202.3 lbs
Overall change showed a starting weight (late December average) of ~207.2 lbs and an ending weight (late February average) of ~202.3 lbs. This resulted in a net loss of ~4.9 lbs, at a rate of ~0.8 lbs per week.
Interpreting the data
When accounting for day-to-day variability, the trend is clear: Weight steadily declined over time. This occurred with just one intervention, eliminating late-night caloric intake. There was no dietary overhaul. There was no new exercise regimen. There was just consistency.
I was not surprised that the intervention worked. I was surprised by how volatile the daily numbers were. It took grit to stay steady on mornings when the scale suggested I had gained four pounds overnight. Yet those spikes did not persist. Conversely, sharp short-term drops were often followed by partial rebounds. Over time, however, each successive baseline trended lower than the one before. The overall pattern resembled a downward staircase, temporary fluctuations layered over a clear decline.
The psychological shift
Despite its simplicity, this regimen was not easy. At 11:30 p.m., the ER track board would light up, adrenaline would spike, and the urge to snack felt almost automatic. Sometimes I told myself: “Wait until 1:00 a.m. You do not have to eat right now.” Other times, I relied on coffee, water, or diet soda to bridge the gap. Some nights, I came close to breaking the rule. But consistency mattered.
And something interesting happened: after a few days, the fasting window became easier. The urge did not disappear, but it became manageable. I felt more in control of my eating, rather than the other way around. Maybe the critics are right; perhaps I simply shifted calories into a different window. But that “shift” was the point. By removing food from my most vulnerable hours, I removed the habit driving excess intake.
Takeaways for night-shift physicians
- Late-night eating is a significant contributor to weight gain, and even small reductions matter.
- Simple rules outperform complex diets.
- Consistency matters more than perfection.
- Daily weight fluctuations are normal; focus on trends, not single data points.
- The hardest moment is often psychological, not physiological.
Aaron Grubner is a pediatric emergency medicine physician.

































