The May 2, 2026, New England Journal of Medicine (NEJM) Perspective, “From Mission to Margin in Academic Medicine,” articulates an internal struggle I feel frequently. All physicians recognize the formative environment Dr. Vyas describes as something that must be fiercely protected, and his call to action against the commodification of training resonates deeply. As an emergency department physician practicing outside of this setting, I recognize that when we succumb to the pressures and prioritize throughput over thoughtfulness, we model transactionalism and project a version of humanity that is increasingly automated and decreasingly empathetic. Without the institutional buffers of a teaching hospital, self-defense becomes a deliberate protection of purpose. The basis for this discipline began at a breakfast buffet in North Carolina, long before I ever stepped into an ER.
I was a teenager, headed home from summer vacation with my family, and we had just pulled in off the turnpike, a typical scene of American middle-class life. Upon opening the door, a thick, manufactured colloid of smells greeted us: the aggressive sweetness of imitation maple syrup, the greasy perspiration of sausage patties resting in a stainless-steel tray, and the damp, almost sulfurous smell of reconstituted eggs. The glossy food shown on the highway billboard bore little resemblance to the lukewarm fare languishing under the perpetual sun of a string of heat lamps.
It was in this theater of manufactured comfort that my eyes fell on her and stayed. She was the pregnant teenager in the corner, quietly bussing the tables, wearing a uniform not designed for her condition: a tan shirt, brown pants with an elastic waistband that strained under a large brown apron that bulged forward, and a bouffant cap perched on her head. One or two years older than me, at most, and moving with a practiced economy that stood in stark, almost accusatory contrast to the leisurely pace of the patrons whose ketchup-smeared plates she would systematically clear away, mine included. Her pregnancy was an undeniable fact in the room, and I could almost hear the silent, frictionless judgments forming around her, the swift, easy categorization of her entire existence by people who would forget her face before they returned to their cars.
I could only imagine, without presuming to know, the challenges she faced, since my entry into the workforce earlier that summer carried none of the existential weight hers clearly did. A few days later, I resumed my first foray into gainful employment, painting and refurbishing classrooms at my high school. As someone accustomed to the easy recognition that came with being a straight-A student, I was learning that a specific style of attire (paint-splattered jeans, a shirt you don’t care about, and a backward baseball cap) can render you practically invisible to a certain type of person. In those moments, I sensed a sympathetic resonance with her, a phantom echo of that same erasure. People I knew would look at me, and their eyes would slide away, as if I were a piece of lawn decor. I soon realized my invisibility was temporary, a costume I would shed at the end of the day. Once I had showered and changed, it was back to business as usual, being a privileged suburban teenager in an affluent hamlet of Westchester County, New York, a place called, with near-perfect irony, Pleasantville.
Our encounter that summer later became tangled with a persuasive essay I was assigned in my Honors English class on abortion. What could I, a fifteen-year-old virgin sheltered in the comforts of suburban life, say that wasn’t borrowed or feigned? My opinions felt unearned. I could research statistics or parrot arguments, but I couldn’t possibly grasp the lived reality behind what I witnessed at the restaurant in North Carolina. The girl in the diner wasn’t a case study or a talking point; she was living the reality of the words we were asked to conjure on paper. In just under two pages, I described what happened, how I felt, and concluded that I could only admit my profound uncertainty in the face of another person’s real-world experience and would therefore keep my mouth shut on the subject. When the paper was returned, written in red ink at the top of the page were the words: “The most honest answer I’ve ever read.”
I didn’t realize then that the “honesty” of that uncertainty would become a vital clinical tool I would strive to protect as an adult. In the twenty years since completing residency, the tension described in the NEJM Perspective has become my daily reality: the relentless priority of “margin” over “mission” colliding with the messy, unknowable lives of my patients. In a community hospital, this tension carries particular weight; we lack the buffers of tradition or altruism that the academic setting might otherwise offer. Instead, the focus on metrics and getting the work done leaves us more vulnerable to ever-increasing demands and to acting almost instinctively. While operating in turbulent environments with multiple competing stimuli, our brains are wired to flatten complex, competing realities into a single, digestible narrative, a cognitive reflex best illustrated by the famous “Young Woman, Old Woman Ambiguous Figure” optical illusion from an 1888 German postcard.
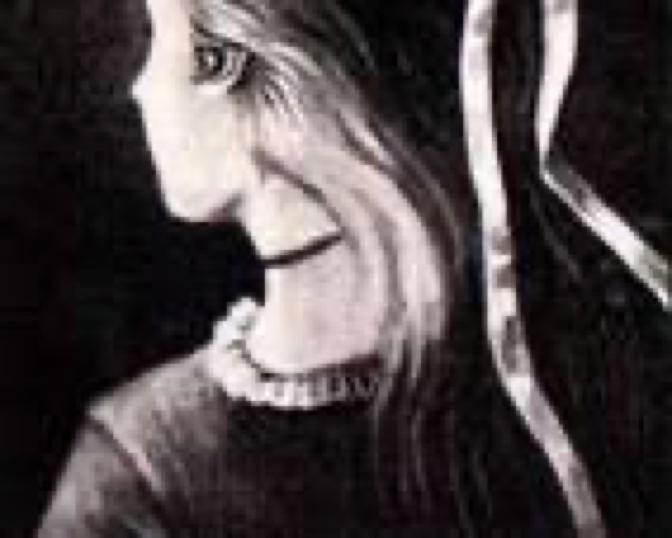
The mechanics of this illusion are explained by the Gestalt switch, the sudden mental leap in which our perception flips. When the initial impression generated by early-stage visual processing centers is actively suppressed, an “aha” moment occurs, reorganizing the same ocular input into a second, distinct interpretation.
The image of her quietly bussing tables, my own application of the Ambiguous Figure, now serves as a permanent, internal gut check. It’s the fire alarm etched into my brain I can pull whenever the pressure of “the margin” feels insurmountable. In a simple act of quiet resistance, I force the image of her to the surface before I knock on the door of my next patient. This pause reminds me to separate the conscious, internal labor of understanding another’s experience from the reductive certainty of labels like “the STEMI in 14,” “the woman in 3 with the PE,” or “the hemorrhagic stroke from CT.”
It is a discipline born of a chance encounter at a highway breakfast stop. Forever an “Ambiguous Figure,” she remains my touchstone, a conscious push to see past first impressions and to hold on to the discipline of uncertainty, one patient encounter at a time.
Michael Schmitz is a board-certified emergency department physician who has practiced in Maine since July 2008. He completed the dual emergency medicine and internal medicine residency at St. Barnabas Hospital in the Bronx, and he currently practices at MaineHealth-Midcoast Hospital and Houlton Regional Hospital as part of BlueWater Emergency Partners. He is proud to be part of a culture that actively works to normalize the conversation around the tension between mission and margin, ensuring that a shared sense of purpose remains at the forefront of high-quality clinical practice.
His writing has appeared in MedPage Today, the Portland Press Herald, EMSWorld, and ROOM: A Sketchbook for Analytic Action, with a focus on physician well-being, public health, and the lived experience of clinical practice. A representative sample of his work includes “Can we please stop calling it burnout?,” “Maine Voices: York County vaccine clinic was a master class in local teamwork,” and “An open letter to my paramedic students.” He has also appeared as a guest and panelist on Maine Public Radio’s Maine Calling, discussing COVID-19 vaccine distribution and health care worker burnout.
He lives in Maine with his wife, five children, three dogs, two cats, and a horse, and remains an unapologetic fan of the 27-time World Champion New York Yankees. He can be found on LinkedIn.






























